Sunday, November 26, 2006
Total knee replacment video of British patient in India
>Watch this video of a British patient settled in Spain. Observe the Pre op gait, careful pre op planning, execution and deep knee bending achieved on the table in this High flex knee replacement. Contact 00 91 9282165002 or mail akvenkat_19@yahoo.com for an appointment for knee surgery.
Sunday, November 05, 2006
Bilateral knee replacements for Kenyan grandfather in Chennai


This 67 year old Somalian citizen, a resident of Kenya had bilateral knee replacements for grossly damaged and osteoarthritic knees. He had severe flexion contactures as seen in the pre op photo to the left and this was corrected after surgery.
For Bilateral knee replacements under one anesthetic, please contact 00 91 9282165002 or e mail akvenkat@gmail.com
Saturday, October 21, 2006
Pre Op planning for a total knee replacement
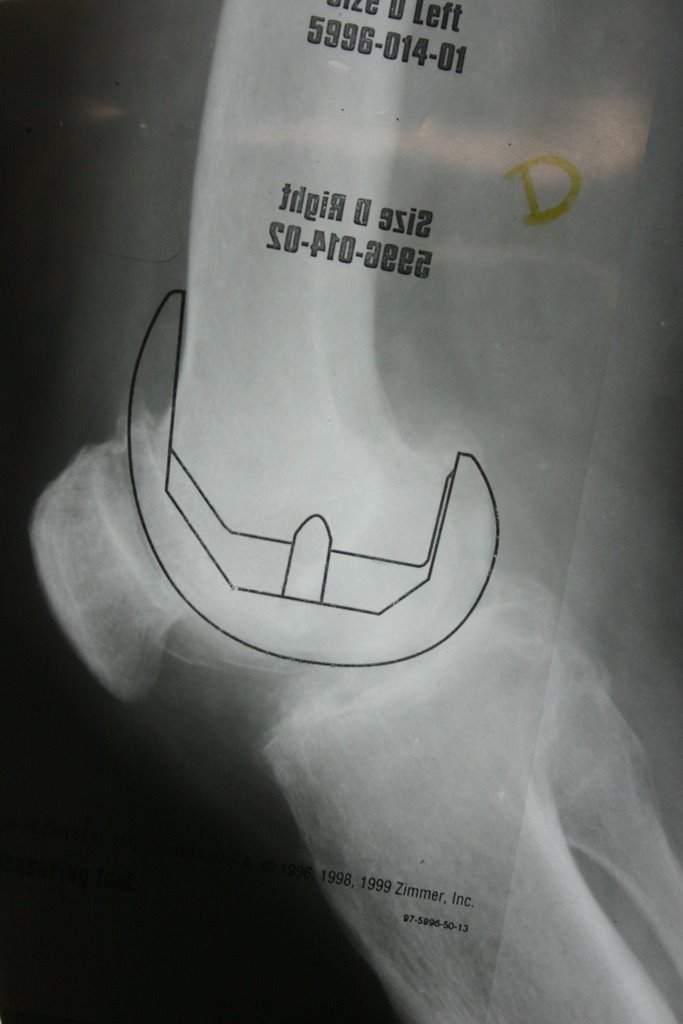

Accompanying x ray shows careful pre op plannning for a total knee replacement which allows the surgeon to choose the right size of the prosthesis.
Monday, October 16, 2006
Deep Knee bending for climbing stairs
 Lady with bilateral knee replacements climbing stairs on 5th Post Op day. Visit www.kneeindia.com for more information on cost effective bilateral High flex knee replacements or mail the surgeon at akvenkat@gmail.com.
Lady with bilateral knee replacements climbing stairs on 5th Post Op day. Visit www.kneeindia.com for more information on cost effective bilateral High flex knee replacements or mail the surgeon at akvenkat@gmail.com.
Sunday, October 01, 2006
Watch Video of Total knee replacement
here
Hit the Play button
Video shows advantages of the High flex knee replacement with a fixed bearing knee.
For appointments or quote on knee replacement e-mail me at akvenkat@gmail.comknee replacement video
Oxford Knee replacement video India
Watch Video of Partial knee replacement here
Hit the Play button or symbol
This video shows how a patient returns to normal function within a week after bilateral Oxford mobile bearing partial knee replacements.
For an appointment to have your knee surgery, mail me at akvenkat@gmail.com
Tuesday, September 12, 2006
Bilateral Knee replacements with High flex knee
 The above oicture shows a lady sitting cross legged three months after bilateral High flex knee replacement
The above oicture shows a lady sitting cross legged three months after bilateral High flex knee replacementA double knee replacement using the Nex gen High flex knee was performed on this 68 year old houssewife for osteoarthritis. Knee expert Dr.Venkatachalam performed the operation at a private hospital in Chennai.
Citing that bilateral replacements were pioneered by him in the city since the last few years, Dr.Venkatachalam, said that the procedure had several advantages. Firstly it involved only one hospitalisation for the patient with bilateral knee disease. There was only one recovery, anesthesia and one surgery. Off course the whole exercise is a lot more economical than having two knees operated upon separately.
The Pre op condition of the patient is most important as he or she should be fit to undergo prolonged anesthesia and surgery.
People suffering from Rheumaotid arthritis are greatly benefitted by bilateral Knee replacements as their misery of wheel chair confinement comes to an end with the surgery.
Citing that bilateral replacements were pioneered by him in the city since the last few years, Dr.Venkatachalam, said that the procedure had several advantages. Firstly it involved only one hospitalisation for the patient with bilateral knee disease. There was only one recovery, anesthesia and one surgery. Off course the whole exercise is a lot more economical than having two knees operated upon separately.
The Pre op condition of the patient is most important as he or she should be fit to undergo prolonged anesthesia and surgery.
People suffering from Rheumaotid arthritis are greatly benefitted by bilateral Knee replacements as their misery of wheel chair confinement comes to an end with the surgery.
Thursday, September 07, 2006
Squatting knee or High flex Total knee replacement -Indian Lady squatting after 3 months
 Only the High flex knee or sqatting knee allows full function in activities like deep knee bending, kneeling, squatting, praying etc. The Rotating platform knee cannot achieve 155 degrees of bending. South Indians Hindus, Muslims and Christians are very thankful for the full function allowed by a High flex knee.
Only the High flex knee or sqatting knee allows full function in activities like deep knee bending, kneeling, squatting, praying etc. The Rotating platform knee cannot achieve 155 degrees of bending. South Indians Hindus, Muslims and Christians are very thankful for the full function allowed by a High flex knee.For a quote on High flex Knee replacement please send me mail at akvenkat@gmail.com
Tuesday, September 05, 2006
Can your Knee replacement achieve this?
This 67 year old Doctor is the first patient to undergo a High flexion Knee replacement in India. The surgery was performed by DR.A.K.Venkatachalam, consultant Orthopedic surgeon of www.kneeindia.com. Six months after the surgery he has regained full flexion and offers prayers five times a day. In his words he can drive, walk, kneel fully and pray.To achieve this, the patient should be willing to participate in aggressive physio.
Kindly see post " First high flex knee replacement " also.
If you want more details or a quote for any Knee surgery, you can mail at akvenkat@gmail.com
Sunday, August 27, 2006
Is knee arthritis inevitable with aging?
This is the common perception of Knee Osteoarthritis in India where Primary Hip Osteoarthritis is rare. However in the recent past, it has been realized that not only are the elderly at definite risk of Osteoarthritis but many more of the middle aged and even young. Osteoarthritis is the commonest form of joint disease (arthritis) and is a leading cause of disability in older individuals in India and many countries. It is the common perception that wear and tear inevitable with aging alone leads to Osteoarthritis, but this is not the whole truth. As we shall see not only the elderly, but others are also vulnerable to Osteoarthritis.
Osteoarthritis (OA) in peripheral joints, most frequently involves the knee joint, and the disease may affect one or more of the three compartments of the knee. The knee joint acts to transfer force from the thigh muscles to the leg to move the body. Loads exerted on the surfaces of the knee during normal daily activities are two to seven times the body weight. It is therefore no wonder that the knee is so vulnerable to wear and tear (Osteoarthritis). Osteo-arthritic changes in the joint decrease the effectiveness of load transfer during these activities. Overall health is impaired and Knee OA has been to shown to account for more limitations in walking, stair climbing or other daily activities than any other disease. The form of the disease in the elderly is called primary osteoarthritis whereas the affliction of the young and middle aged is called Secondary osteoarthritis. Let us take a look at the risk factors for developing secondary osteoarthritis, which encompasses other age groups of people in the general population.
These are of two categories, General or systemic and local risks.
General risks
Evolution
Man along with two more mammals, the Elephant and the bear are the only animals to have straight knees. Evolutionarily straight knees are invaluable to minimize energy expenditure during walking so that the body does not tilt from side to side as it would do if the knees were bent in a two legged creature. The price or side effect of the erect posture is weight transmission occurring through the inner half of the knee joint. Therefore the inner half of the knee is susceptible to wear in the normal course of time.
Genetic factors
These play a major role in a generalized form of the disease known to affect some communities and families. Research is on to identify the exact genetic location that increases the susceptibility to OA.
Diet
Many degenerative diseases like Osteoarthritis are the result of tissue damage from “Free Oxygen radical” attack. Normal cartilage cells are known to reduce free radicals. Anti oxidants such as Vitamin A, C and E have the potential to protect against such tissue damage. It was found in a study that people consuming High amounts of Vitamin C have a 60- 70 per cent reduction in risk for progressive OA. High vitamin C intake levels were also found to be associated with a reduced risk for knee pain according to the same study.
Vitamin D plays an important role in bone mineralization. Results from the above study show that high levels are protective against progression of disease.
Bone mineral density
About three decades ago surgeons removing the head of the upper end of the thigh bone from elderly patients with hip fractures in the operation of partial hip replacement, observed that the end bone rarely showed arthritic changes. Since then, many studies have confirmed the inverse relationship between Osteoporosis and Osteoarthritis. Currently research is on to determine if the medicines prescribed for Osteoporosis such as Calcitonin and Bisphoshphonates prevent the x- ray changes of OA and prevent cartilage breakdown.
Female hormonal deficiency (estrogen)
The incidence of Knee OA increases in Post menopausal women suggesting that estrogen deficiency might be a risk factor and that post menopausal women are more susceptible to osteoarthritis. Despite the obvious correlation, more research is needed to understand the relationships between bone mineral density, estrogen and OA. As females are the preponderant sex to suffer from OA knees, Female specific Knee implants or Prostheses have been developed for a Total knee replacement as the majority of people (two thirds) undergoing a knee replacement are women.
Local risk factors
Obesity
Increased body weight contributes to the increased load transmitted across the weight bearing knees by a factor of three to seven times the body weight and leads to accelerated wear of the articular cartilage. The relationship between obesity and Osteoarthritis is stronger for bilateral than unilateral disease and is greater in women than men. Since the load transmitted to the knees varies between three to seven fold the body weight, one fold reduction of weight leads to a three to seven fold decreased pressure on the knees. In addition the knee alignment may affect the impact of body weight on the knee joint. Knees with bow legs are more stressed by body weight resulting in more severe inner compartment arthritis.
Physical activity
There is no evidence that participation in light or moderate levels of physical activity (walking, running, dancing, cycling, gardening, and outdoor sports) throughout the life cycle will increase an individual’s risk of developing knee OA. This means that even middle aged people can safely participate in these activities without risk of developing osteoarthritis.
However participation in high intensity contact sports is strongly linked to development of knee OA in elite athletes. Many tennis players, runners, professional soccer players are more likely to suffer from knee arthritis and Patello-femoral OA than age matched controls.
Occupational activity
Men in occupations that require repetitive overuse of the knee joint for example, carpenters, painters, miners, dock workers have an increased risk of developing knee OA. Crouching, kneeling, squatting, climbing stairs and lifting heavy loads all cause abnormal joint loading across the knee joint and lead to cartilage damage. The risk factors are similar in both men and women.
Injury
Several studies in Europe and America have confirmed that knee injury is a strong predictor for the development of knee OA. Most Knee injuries involve the ACL (Anterior cruciate ligament and ACL rupture is often associated with meniscal damage or a tear in the medial collateral ligament. ACL injuries occur after two wheeler accidents, domestic and outdoor accidents. Both ACL deficiency and meniscal rupture are strongly linked to early degenerative arthritic changes. Although at present it is not clear to what extent the common operation of ACL reconstruction can delay the onset of arthritis, some studies show that early ACL reconstruction with meniscal preservation and not menisectomy provides the greatest protection. A poor outcome after knee injuries is seen in patients who have undergone a partial or total menisectomy an operation which is commonly performed by surgeons. Meniscal suture and Meniscal transplant are ways to protect against osteoarthritis. The former operation is available but the later is yet to kick off from early teething problems. A meniscal transplant facility was announced in Chennai last year but supply of grafts has not been forthcoming.
Mechanical environment of the knees
It is easy to comprehend how any joint or bearing can wear out quickly by understanding what happens to your car tyres if the alignment and balancing is not perfect or if the pressure is more or less. The treads on the overloaded portion of the tyre wear out more. The same analogy applies to the knees. Knees which have a bend like the one shown in the picture will wear out faster. Increased joint laxity an accompaniment of age contributes to OA.
Muscle strength
It is a well known observation that people with OA have weakness of the quadriceps muscles. It was assumed that decreased muscle strength is the result of disuse atrophy secondary to knee pain; however it has been noted recently that many patients with asymptomatic knee arthritis have weak muscles. Therefore it makes sense to develop the thigh muscles to prevent arthritis or ameliorate the symptoms after its development, but is to be noted that increasing muscle strength will not arrest progression of the disease.
In summary Knee Osteoarthritis once considered an inevitable consequence of aging is now recognized to be multi-factorial, resulting from the interaction of a variety of general and local factors like age, genetic predisposition, obesity, trauma and mechanical properties of the joint. The traditional surgical treatment of OA “a total knee replacement” is the best long term cost effective solution. However other operations like an osteotomy to correct the alignment of the bones around the knee, ACL reconstruction, cartilage surgery, medications are available to different affected groups of patients. They will not condemn the patient to developing Osteoarthritis in earlier age and become a candidate for a total knee replacement.
Osteoarthritis (OA) in peripheral joints, most frequently involves the knee joint, and the disease may affect one or more of the three compartments of the knee. The knee joint acts to transfer force from the thigh muscles to the leg to move the body. Loads exerted on the surfaces of the knee during normal daily activities are two to seven times the body weight. It is therefore no wonder that the knee is so vulnerable to wear and tear (Osteoarthritis). Osteo-arthritic changes in the joint decrease the effectiveness of load transfer during these activities. Overall health is impaired and Knee OA has been to shown to account for more limitations in walking, stair climbing or other daily activities than any other disease. The form of the disease in the elderly is called primary osteoarthritis whereas the affliction of the young and middle aged is called Secondary osteoarthritis. Let us take a look at the risk factors for developing secondary osteoarthritis, which encompasses other age groups of people in the general population.
These are of two categories, General or systemic and local risks.
General risks
Evolution
Man along with two more mammals, the Elephant and the bear are the only animals to have straight knees. Evolutionarily straight knees are invaluable to minimize energy expenditure during walking so that the body does not tilt from side to side as it would do if the knees were bent in a two legged creature. The price or side effect of the erect posture is weight transmission occurring through the inner half of the knee joint. Therefore the inner half of the knee is susceptible to wear in the normal course of time.
Genetic factors
These play a major role in a generalized form of the disease known to affect some communities and families. Research is on to identify the exact genetic location that increases the susceptibility to OA.
Diet
Many degenerative diseases like Osteoarthritis are the result of tissue damage from “Free Oxygen radical” attack. Normal cartilage cells are known to reduce free radicals. Anti oxidants such as Vitamin A, C and E have the potential to protect against such tissue damage. It was found in a study that people consuming High amounts of Vitamin C have a 60- 70 per cent reduction in risk for progressive OA. High vitamin C intake levels were also found to be associated with a reduced risk for knee pain according to the same study.
Vitamin D plays an important role in bone mineralization. Results from the above study show that high levels are protective against progression of disease.
Bone mineral density
About three decades ago surgeons removing the head of the upper end of the thigh bone from elderly patients with hip fractures in the operation of partial hip replacement, observed that the end bone rarely showed arthritic changes. Since then, many studies have confirmed the inverse relationship between Osteoporosis and Osteoarthritis. Currently research is on to determine if the medicines prescribed for Osteoporosis such as Calcitonin and Bisphoshphonates prevent the x- ray changes of OA and prevent cartilage breakdown.
Female hormonal deficiency (estrogen)
The incidence of Knee OA increases in Post menopausal women suggesting that estrogen deficiency might be a risk factor and that post menopausal women are more susceptible to osteoarthritis. Despite the obvious correlation, more research is needed to understand the relationships between bone mineral density, estrogen and OA. As females are the preponderant sex to suffer from OA knees, Female specific Knee implants or Prostheses have been developed for a Total knee replacement as the majority of people (two thirds) undergoing a knee replacement are women.
Local risk factors
Obesity
Increased body weight contributes to the increased load transmitted across the weight bearing knees by a factor of three to seven times the body weight and leads to accelerated wear of the articular cartilage. The relationship between obesity and Osteoarthritis is stronger for bilateral than unilateral disease and is greater in women than men. Since the load transmitted to the knees varies between three to seven fold the body weight, one fold reduction of weight leads to a three to seven fold decreased pressure on the knees. In addition the knee alignment may affect the impact of body weight on the knee joint. Knees with bow legs are more stressed by body weight resulting in more severe inner compartment arthritis.
Physical activity
There is no evidence that participation in light or moderate levels of physical activity (walking, running, dancing, cycling, gardening, and outdoor sports) throughout the life cycle will increase an individual’s risk of developing knee OA. This means that even middle aged people can safely participate in these activities without risk of developing osteoarthritis.
However participation in high intensity contact sports is strongly linked to development of knee OA in elite athletes. Many tennis players, runners, professional soccer players are more likely to suffer from knee arthritis and Patello-femoral OA than age matched controls.
Occupational activity
Men in occupations that require repetitive overuse of the knee joint for example, carpenters, painters, miners, dock workers have an increased risk of developing knee OA. Crouching, kneeling, squatting, climbing stairs and lifting heavy loads all cause abnormal joint loading across the knee joint and lead to cartilage damage. The risk factors are similar in both men and women.
Injury
Several studies in Europe and America have confirmed that knee injury is a strong predictor for the development of knee OA. Most Knee injuries involve the ACL (Anterior cruciate ligament and ACL rupture is often associated with meniscal damage or a tear in the medial collateral ligament. ACL injuries occur after two wheeler accidents, domestic and outdoor accidents. Both ACL deficiency and meniscal rupture are strongly linked to early degenerative arthritic changes. Although at present it is not clear to what extent the common operation of ACL reconstruction can delay the onset of arthritis, some studies show that early ACL reconstruction with meniscal preservation and not menisectomy provides the greatest protection. A poor outcome after knee injuries is seen in patients who have undergone a partial or total menisectomy an operation which is commonly performed by surgeons. Meniscal suture and Meniscal transplant are ways to protect against osteoarthritis. The former operation is available but the later is yet to kick off from early teething problems. A meniscal transplant facility was announced in Chennai last year but supply of grafts has not been forthcoming.
Mechanical environment of the knees
It is easy to comprehend how any joint or bearing can wear out quickly by understanding what happens to your car tyres if the alignment and balancing is not perfect or if the pressure is more or less. The treads on the overloaded portion of the tyre wear out more. The same analogy applies to the knees. Knees which have a bend like the one shown in the picture will wear out faster. Increased joint laxity an accompaniment of age contributes to OA.
Muscle strength
It is a well known observation that people with OA have weakness of the quadriceps muscles. It was assumed that decreased muscle strength is the result of disuse atrophy secondary to knee pain; however it has been noted recently that many patients with asymptomatic knee arthritis have weak muscles. Therefore it makes sense to develop the thigh muscles to prevent arthritis or ameliorate the symptoms after its development, but is to be noted that increasing muscle strength will not arrest progression of the disease.
In summary Knee Osteoarthritis once considered an inevitable consequence of aging is now recognized to be multi-factorial, resulting from the interaction of a variety of general and local factors like age, genetic predisposition, obesity, trauma and mechanical properties of the joint. The traditional surgical treatment of OA “a total knee replacement” is the best long term cost effective solution. However other operations like an osteotomy to correct the alignment of the bones around the knee, ACL reconstruction, cartilage surgery, medications are available to different affected groups of patients. They will not condemn the patient to developing Osteoarthritis in earlier age and become a candidate for a total knee replacement.
Saturday, July 01, 2006
Lateral release for Patellar(Knee cap) dislocation and pain
| Video shows an arthroscopic LASER assisted lateral release of the lateral retinaculum for patellar dislocation and patello femoral arthritis. The same can be performed using a radiofrequency device at the Knee & Shoulder centre, Chennai. Visit www.kneeindia.com | |
Wednesday, June 07, 2006

Saturday, May 27, 2006
Tuesday, May 16, 2006
High flex knee replacement for British lady in Chennai

A High flex Knee replacement was performed for this sweet lady from North east England last week by Dr.A.K.Venkatachalam of www.kneeindia.com
British lady skips NHS wait- Has knee replaced in Chennai

A 69 year old lady from North east England has skipped the NHS wait by having her knee replaced by Dr.Venkatachalam last week. Here she is seen bending her knee beyond 90 degrees on the fourth day after surgery.
Friday, April 21, 2006
Why you should have your Knee replacement in Chennai ?


The numbers of people searching the internet for knee surgery in India is increasing by leaps and bounds each day. These people hail from the UK, US, New Zealand, Canada, Middle east and India.
Knee replacement at the Knee & Shoulder clinic, Chennai is cost effective, and performed to the latest trends as in the west. Some of the recent advances in Knee replacement are incorporated, thus maximising patient expectations and comfort. Minimally invasive knee surgery, High flex TKR, Quads sparing approaches, to name a few are latest advances. Patient testimonials from the UK, US and other countries vouch for our skills and abilities. An example of the High flex Knee implanted in this patient demonstrates that maximum flexion has been achieved in the right operated knee.
We do not have any agents, relying only on testimonials and recommendations of our satisfied patients, thus keeping all costs to the minimum actuals.
The hospitals where surgery is performed have laminar air flow which reduces the incidence of infection. Our packages are one of the most affordable cost wise and in standards surpass the others.
Anesthetists work in close tandem with the patient to alleviate pain.
Physiotherapists who have trained at some of the Joint replacement centres in the US will be available to help you to regain function at the earliest.
The ambience of the hospitals will be pleasing and at the conclusion of successful surgery, you will be guided to explore the rich cultural and architectural heritage of South India. A rejuvenating Ayurvedic package is available for relatives and patients.
Wednesday, April 19, 2006

Thursday, April 13, 2006
Electro surgical treatment for cartilage lesions

Mr.WR, An American underwent bilateral arthroscopic surgery for patellar and knee cartilage lesions.
Although he is only 28 years old, martial arts practice had lead to fissuring of his knee cap's cartilage. This was treated by the new technique of Electro-cautery in which a radiofrequency device is applied to the swollen areas to shrink the deep layer of damage. Stable edges were achieved by careful mechanical means.
Having lost a lot of weight, he utilised this opportunity of availing Cosmetic surgey under the same anesthetic.
Visit www.kneeindia.com for more information on Knee problems.
Tuesday, April 11, 2006
Orthopedic surgery in India for UK, USA citizens - Chennai favorite destination

www.kneeindia.comPatients from the UK, USA, Australia and Canada needing surgery abroad find Chennai’s skilled orthopedic surgeons, affordable costs and clean private hospitals a safe haven. Absence of hidden costs and agents, transparent dealings, skilled surgery, nursing, physiotherapy, clean hospitals are factors responsible for increasing medical treatment abroad says consultant orthopedic surgeon, Dr.A.K.Venkatachalam of Bharathi raja speciality hospital, Chennai.Patients find doctors by word of mouth and the internet. Knee & Hip replacements, Surface hip replacement, shoulder surgery are some sought after operations.
Emerging collapse of Medicare in the US and the NHS in the UK are forcing ordinary folk to seek orthopedic medical treatment in India. Elderly people with chronic orthopaedic problems like Hip and knee osteoarthritis, shoulder and spine problems are unable to withstand their pain and cannot afford private treatment in their own countries. They discover well qualified and trained Indian doctors performing these operations in India at affordable costs and hence prefer Private treatment in Chennai.
Dr.Venkatachalam is a consultant orthopedic surgeon in Chennai's Bharathiraja specialty hospitals. He has treated patients from the UK, US, Greece, Spain, UAE, Quatar, Bangladesh and South Asia for knee and shoulder problems. He pioneered High flexion knee replacements with the only implant designed for the purpose.
Having worked in the West earlier enables doctors to understand the requirements of their patients in terms of comfort, standard of care, communication, food habits of the patients etc. Westerners find themselves comfortable in the presence of UK qualified doctors. The common operations like total knee & hip replacements, hip resurfacing, arthroscopic surgery of shoulder and knee are much in demand amongst these medical tourists. While emergency care is excellent in the UK’s NHS, patients are faced with long waiting lists of up to a year for elective orthopedic surgery. Having paid up their tax contributions they become frustrated when they cannot get timely surgical treatment for chronic joint problems. Unlike patients with heart disease, people with orthopaedic problems can travel safely and are doing exactly that, flying half way around the world to India for orthopedic surgery.
Mark Carr, an outdoor sports expert from Wales who underwent shoulder surgery in Chennai six months ago, says “When recently faced with a further 12 months of shoulder pain and the resultant inactivity, I decided to look for a solution outside the NHS. Of course there is private surgery in the UK. I asked the cost and was told £4500. This was more than I could afford. Back to search the web. Links led me to Dr A. K. Venkatachalam who is based in Chennai India and who is a very highly qualified Orthopaedic Surgeon who trained in the UK and has worked in several major hospitals in Asia and the Middle East. My operation was skillfully performed, I know that because I have seen the photographs and am now enjoying the results. After ten days the constant nagging pain that had been with me for more than a year had gone and I enjoyed my first full night’s sleep for that same period.”
The same kind of frustration and inability to earn income and lay off from work due to pain arising from Knee osteo-arthritis also drove Mr. Brian Toughton, a 66 year old luxury coach driver from Stratford upon Avon to seek a knee replacement in Chennai. He came to have only one knee replaced, but when he realized that he couldn’t afford another trip for surgery to his other knee which was also in the same diseased state; he decided to have bilateral knee replacements done. He did not regret it and was able to enjoy a fortnight’s holiday in a seaside resort.
Concerns amongst patients about cleanliness of hospitals, skills of surgeons, and familiarity of latest techniques are put to rest easily as Mr. Cliff Arkley, a marine consultant from Sussex found out recently by his experience. This gentleman underwent bilateral partial knee replacements. The prosthesis inserted was Unicondylar prosthesis with a mobile bearing. The surgery was performed through 3 inch long incisions called minimally invasive surgery or MIS.
Advantages of minimally invasive surgery are decreased blood loss, lesser operating time and morbidity, less pain, quick rehabilitation and return of function. MIS, high flexion knee replacements ( allowing more natural bending of the knee to 155 degrees) are some of the latest advances in knee surgery available in the west and foreigners are delighted to have the same performed in India for a fraction of the cost.
Affordable Costs - A total hip replacement in the US costs $39000, whereas one in Chennai costs only $6500 along with the cost of the implant. A TKR in the UK costs 9500 pounds whereas the same can be done here for 3500 pounds.
Cost differences are enormous. Dave Hurd an American citizen from North Carolina had to shell out only one tenth of the cost that he paid in the US for a rotator cuff repair in India.
Patients find it easier to pay out of pocket than claim insurance. These surgical options are attractive and patients are lining up to have their orthopaedic surgery performed in Chennai.
An added attraction at the successful conclusion of their surgery is recuperation in nearby resorts and spas. This added comfort mitigates to some extent the absence of loved ones by their side during recovery. At the conclusion of successful treatment, patients can choose to tour more of India before retuning home. The charms of Kerala's back waters, the idyllic beaches of Goa, temples of Tamil nadu, etc are must see attractions in South India.
# # #
Sunday, April 09, 2006
First Japanese medical tourist has knee arthroscopies and cosmetic surgery in India
A 28 year old Alsakan School teacher settled in Japan, has undergone bilateral Knee surgery and Cosmetic surgery in Chennai by www.kneeindia.com's orthopedic surgeon Dr.A.K.Venkatachalam and DR.T,C Chandran, a renowned Plastic surgeon over here.
WR, is a martial arts instructor and developed bilateral knee problems on the undersurface of his knee cap. The risk factors were that he was obese earlier and this had put a lot of pressure on his knees. When he reduced his weight, there was extra skin in his abdomen.
In a six hour long surgery, both the knees were treated by arthroscopic surgery and the reduntant abdominal skin was trimmed to give him a new look which he will be proud to display to his mates back home.
He is recovering well and will be discharged in 3- 4 days from hospital and wil be fit to travel to America.
WR, is a martial arts instructor and developed bilateral knee problems on the undersurface of his knee cap. The risk factors were that he was obese earlier and this had put a lot of pressure on his knees. When he reduced his weight, there was extra skin in his abdomen.
In a six hour long surgery, both the knees were treated by arthroscopic surgery and the reduntant abdominal skin was trimmed to give him a new look which he will be proud to display to his mates back home.
He is recovering well and will be discharged in 3- 4 days from hospital and wil be fit to travel to America.
Monday, March 06, 2006
ACL Reconstruction surgery in middle age

Middle aged and elderly patients with a definite history of symptomatic ACL(Anterior cruciate ligament) tear or injury can benefit from an ACL reconstruction. The Knee is stabilised and further damage to the menisci and articular cartilage of the knee will be prevented. If articular cartilage damage has occured, then the reparative cartilage surgery methods can be combined for focal cartilage defects.
ACL reconstruction has a definite role in the elderly sports person or health conscious person who wants to keep fit by jogging, outdoor activities.
Several sports and fitnees oriented people from the UK and US are now keen to undergo surgery in Chennai, India. ACL repair is another possibility.
The cost of ACL surgery in India being one tenth to one fifth the cost in the USA and UK, is the main factor in drawing patients. Mr.James Sperk says.
"The main attraction for me in getting my surgery done in India was that reduced costs meant that I could use my savings to pursue my hobbies as passionately as before"The adjacent picture shows the reknowned American Mountaineer ( 59 years old) who had undergone an Arthroscopic ACL reconstruction recently.
Visit www.kneeindia.com
Wednesday, March 01, 2006
Arthroscopic ACL Reconstruction in Chennai

http://www.kneeindia.com- ACL reconstruction in Chennai- Sportsmen with ligament and cartilage injuries can develop secondary osteoarthritis if they continue to participate in the sport without rectifying the damage. ACL reconstuction and meniscal repair or transplant is an ideal treatment to avoid knee arthritis. I perform arthroscopic ACL reconstruction using autografts. A meniscal transplant facility is also in place in Chennai with arrangements to procure menisci from cadaveric donors and for storage. I already have few patients on my waiting list for a transplant. When the supply of donor menisci improves, the operation of meniscal transplant will gain momentum.
Sunday, February 26, 2006
ACL reconstruction for Bangladeshi patients

A few patients from Bangladesh recently underwent ACL reconstruction in Chennai. They came from different cities and professions. These included an Army officer, a fisheries department officer and an officer from the Export processing zone in Chittagong.
Since there are no facilities in Bangladesh, they choose to visit India. One of them also appeared on the new TV channel CNN IBN. during his stay in the Chennai hospital. Talking from his hospital bed, Mr.TH, the patient says "
It is not only the operation but the personalised post operative care that makes surgery from this Doctor worth having."
Saturday, February 25, 2006
High flex knee replacement India

The first High flex knee replacement in India was done in Chennai with the only prosthesis designed for the purpose. The Nex gen LPS Flex prosthesis from Zimmer offers deep flexion up to 155 degrees. It is suited to meet the requirements of Indians & middle east citizens. Picture shows amount of flexion achieved after surgery on the operating table itself without any pressure.
Sunday, February 05, 2006
American Everest Hero outsources his orthopedic surgery to India

A mountaineer from the US who has several climbs in Asia, South America including a successful ascent of Mt.Everest has landed up in Chennai's Knee & Shoulder clinic to undergo Knee & Shoulder surgery. He will first have an arthroscopic ACL reconstruction and cartilage surgery to his knee and later have an arthroscopic rotator cuff tear repair.
Once again orthopedic surgery in India is gaining many patients from the West as it is highly affordable, efficacious and prompt.
www.kneeindia.com
www.shoulderindia.com
Tuesday, January 17, 2006
Partial Knee replacement/ reconstruction in India

Unicondylar or Partial Knee replacement in Chennai
Many middle aged men and women develop osteoarthritis of the knee. In Indians Osteoarthritis of the knee affects the inner half or medial compartment to start with. Localized attrition occurs in the beginning. Later on it gradually affects the front and inner portion of the inner half of the knee. This is obvious on standing x rays as a pit or depression.
The standard permanent surgical treatment for osteoarthritis knee has been a total knee replacement. However the ideal candidate for a TKR is a person beyond 65 years, when he can live out the life of an artificial joint which is about 15 years. Says Dr.A.K.Venkatachalam, Knee surgeon of India,
Clearly someone in their fifties is not suited for a TKR as his/her life span would exceed that of the joint and he would need a revision knee replacement later on.Surgical alternatives include an osteotomy and a Uni condylar knee replacement. In an osteotomy, the thigh or leg bone is divided and re aligned so that the abnormal weight bearing axis is normalized. Pain relief is provided for a period of up to 10 years but is not total. It is suited for manual laborers whose work demands would wear out an artificial joint.
A unicondylar knee replacement substitutes the inner worn half of the joint with prosthesis. The bony resection is restricted to the affected half alone sparing the outer half and the patella unlike a total knee replacement. The operation can be done by a minimally invasive technique sparing the quadriceps muscle. The pre requisites are that the inner half alone must be worn as seen on x- rays and the anterior cruciate ligament should be intact. Shorter hospital stay, quicker recovery, small incisions, no blood transfusion, less pain, less cost (vs. TKR) and better function (squatting, kneeling, climbing stairs) are the much acclaimed benefits. The knee feels more natural as sensations carried by the ligaments are intact.
The Oxford unicompartmental knee is a mobile bearing uniknee. Survivorship analysis is 98% at 15 years. The wear of the mobile polyethylene insert is minimal.
In India,
The first bilateral Oxford knee replacements at Chennai's Knee replacement centre were performed recently for a British marine consultant from Sussex,Mr.Cliff Arkley at Venkataeswara hospital, Chennai by Dr.A.K.Venkatachalam, Consultant orthopaedic surgeon. The procedure was performed through small incisions about 3 inches long( see photo)(minimally invasive surgery)(MIS). A Knee cap replacement operation in India only costs one third of that in the UK.
Monday, January 16, 2006

Thursday, January 12, 2006

Thursday, January 05, 2006
Subscribe to:
Posts (Atom)